

Ever since the US Food and Drug Administration (FDA) authorized the emergency use of a specific formulation (10 mcg/0.2 mL) of the Pfizer-BioNTech coronavirus disease 2019 (COVID-19) vaccine for children ages 5 through 11 years, reports of mix-ups with the Pfizer-BioNTech COVID-19 vaccine formulation intended for individuals 12 years and older (30 mcg/0.3 mL) have been pouring in. Most of the mix-ups occurred in outpatient or ambulatory care settings such as public health clinics, community pharmacies, physician practices, and outpatient clinics. Based on reports sent to the ISMP National Vaccine Errors Reporting Program (ISMP VERP) involving hundreds of children, and the fact that adverse event reporting programs do not receive all the actual cases, it is likely that thousands have been impacted. Some children ages 12 and older received the formulation intended for children 5 to 11 years, resulting in underdoses. Other children ages 5 to 11 years received the formulation intended for individuals 12 years and older, resulting in overdoses.
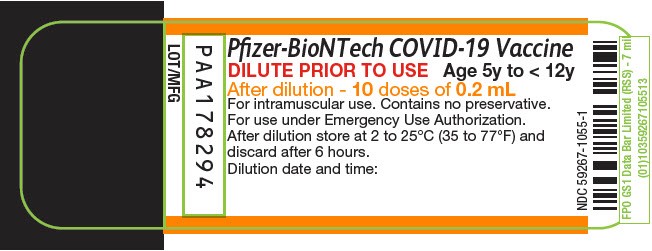
Some errors are due to vial or syringe mix-ups. The label on the pediatric formulation states: “Age 5y to < 12y” (Figure 1), but this is not as prominent as instructions to “DILUTE PRIOR TO USE” and could be missed. Surprisingly, only the injection volume is listed on Pfizer-BioNTech COVID-19 vaccine labels. The dose in mcg is not listed, which would have been helpful in differentiating this product from the 30 mcg/0.3 mL formulation for patients 12 years and older. The 30 mcg/0.3 mL adult formulation vial has a purple cap, while the 10 mcg/0.2 mL pediatric formulation has an orange cap. While different color caps might help prevent some mix-ups, once the cap is removed and discarded, doses may be prepared one at a time rather than all at once, which will render the cap color irrelevant. Also, it is unlikely that the vial will accompany prepared syringes, so the vial label cannot be verified by those administering the vaccine or parents/patients receiving the vaccine.
News media have sometimes reported that parents expressed vaccine hesitancy after hearing about these COVID-19 vaccine errors. Because more than 4 million children ages 5 through 11 have been vaccinated to date, the number of errors described above may seem small in comparison. However, we certainly do not want mix-ups between these vaccine formulations to raise concerns even more and further undermine public health efforts to have as many children vaccinated as possible, even though these errors are not expected to cause serious adverse events, and children receiving underdoses can be revaccinated.
If clinics, physician practices, and/or pharmacies will be administering adult and pediatric COVID-19 vaccines:
-
Develop a plan for segregating and storing the vaccines in refrigerators and freezers that are organized and properly labeled.
-
Store the adult (12 years and older) and pediatric COVID-19 vaccines apart from one another, such as in separate labeled plastic bins.
-
Make it a policy to clearly label all individual syringes containing vaccines. To facilitate proper labeling, the pharmacy should print labels for each patient or provide vaccine preparers with strips of preprinted labels that differentiate adult and pediatric doses. Ideally, prior to administration, barcode scanning should confirm the correct vaccine.
-
When checking in a patient to receive a vaccine, ask the parent or patient to provide at least two patient identifiers—their full name and date of birth. Repeat this process immediately prior to vaccination. For pediatric patients, also verify the patient’s actual age with the parent or caregiver and be sure to ask which vaccine(s) they have requested.
-
Only bring the intended and labeled vaccine syringe(s) for one patient into the vaccination area at a time. Involve the parent or patient in verifying the vaccine by reading the label to confirm the correct vaccine.
-
Document the lot number and date of manufacture prior to vaccine administration, and document administration afterwards in the patient’s profile, on vaccination records, and via state or other immunization registries.
Report all vaccine errors internally as well as to the FDA/CDC (Centers for Disease Control and Prevention) Vaccine Adverse Event Reporting System (VAERS), which is mandatory for COVID-19 vaccine errors under an Emergency Use Authorization (EUA). ISMP also asks providers to report vaccine errors to the ISMP National Vaccine Errors Reporting Program (ISMP VERP). Additional vaccine information can be found here, and in the latest vaccine Fact Sheets for healthcare providers.
The National Alert Network (NAN) is a coalition of members from the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP). The network, in cooperation with the Institute for Safe Medication Practices (ISMP) and the American Society of Health-System Pharmacists (ASHP), distributes NAN alerts to warn healthcare providers about the risk of medication errors that have caused or may cause serious harm or death, or to warn them about new findings that could cause harm and/or are being reported with unusual frequency. NCC MERP, ISMP, and ASHP encourage the sharing and reporting of medication errors both nationally and locally, so that lessons learned can be used to increase the safety of the medication use system.
